909
The sickle of the brain, and 2 models of motion in the craniosacral rhythm for 3 axes
The sickle of the brain, or a sickle large brain and he falx cerebri.
Osteopathy, as you know, an exact science. And as in every exact science in osteopathy simultaneously and equally there are two opposing models of the biomechanics of the sickle of the brain. Will try to disassemble both.
The model of mobility of hammer No. 1
This is a rather mechanistic and very logical model, and it consists in the following.
The sickle of the brain, the tent of the cerebellum and other elements of the Dura mater (dura mater pachymeninx) is a system of membranes of reciprocal tension, or Tensegrity (tensegrity). Sometimes in early translations of foreign osteopathic texts, these elements of Dura mater called the reciprocal of the membrane.
A little of the theory of Tensegrity (tensegrity). A system of mutual tension Tensegrity uses free connection of rigid elements. When exposed to such a system (in our case is gravity, PDM) design changes form. Thus there is redistribution of stresses uniformly over all elements of the system. It provides structural strength, and such a system is obtained simultaneously adaptive and resilient.
By changing the position of the skull bones in the phase of the inflections and extensions of the craniosacral rhythm of the reciprocal tension membrane take the position, so that the voltage is evenly redistributed throughout the system TMO. The tension within the membrane is not changed. I.e. the sickle of the brain and the tent of the cerebellum work as inextensible and elastic membrane.
His own mobility at the sickle of the brain in this model, no no. Shifting to the craniosacral rhythm, cranial bones result in movement of the sickle of the brain and the tent of the cerebellum. The direction and form of the displacement of the membranes are defined by axes and vectors craniosacral mobility of the bones to which these membranes are attached.
Further, it is logical to conclude that examining the biomechanics of the bones associated with the hammer and the tent of the cerebellum, we can understand the biomechanics of the hammer and the tent of the cerebellum.
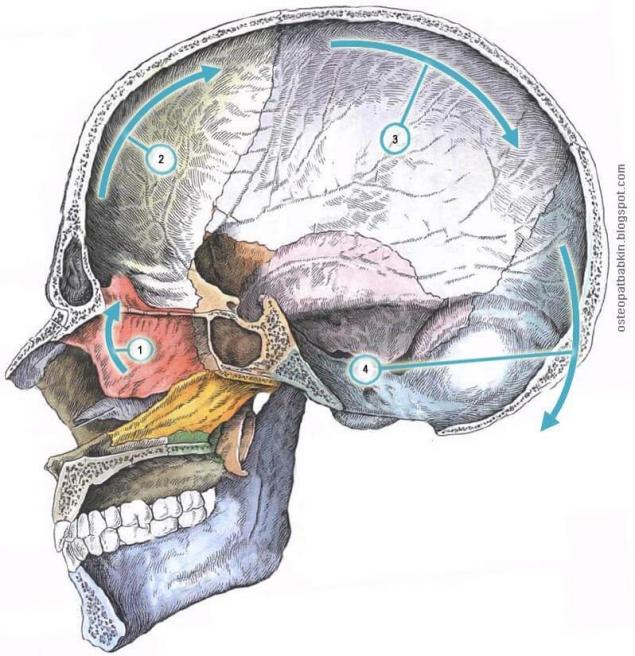
Fig.1. The mobility of the bones of the skull concerned in the movement of the sickle of the brain on the phase of the inflections of the craniosacral rhythm.
1. The sickle of the brain, in its anterior section is attached to the cock the crest of the ethmoid bone.
The movement of the ethmoid bone in the PDM cycle in the sagittal plane:
The movement of the frontal bone on the phase of the inflections of the craniosacral rhythm in the sagittal plane:
The movement of the parietal bones in the PDM cycle in the sagittal plane:
The movement of the occipital bone in the PDM cycle in the sagittal plane:
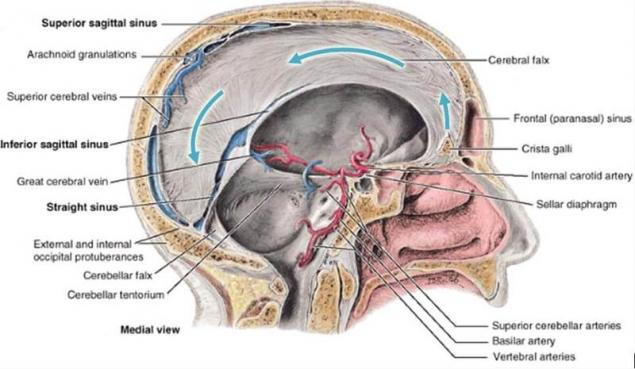
Fig.2. Blue arrows show the movement of a large sickle in the phase of the inflections of VSD.
Model 2, when the hammer twists "on itself"
As we know, Sutherland has put forward 5 phenomena of the primary respiratory mechanism. The classical concept of PDM is based on these five principles:
1. Mailnote the brain and spinal cord. 2. Fluctuations of the cerebrospinal fluid.
3. The mobility of the membranes of reciprocal tension.
4. The mobility of the skull bones in joints.
5. Involuntary mobility of the sacrum between the iliac bones.
The centre of this movement, or fulcrum is the fulcrum of Sutherland, located in front of the straight sinus. This is a moving, dynamic pivot point that moves its position during the cycles of primary respiration. During the phase of exhalation the opposite happens movement.
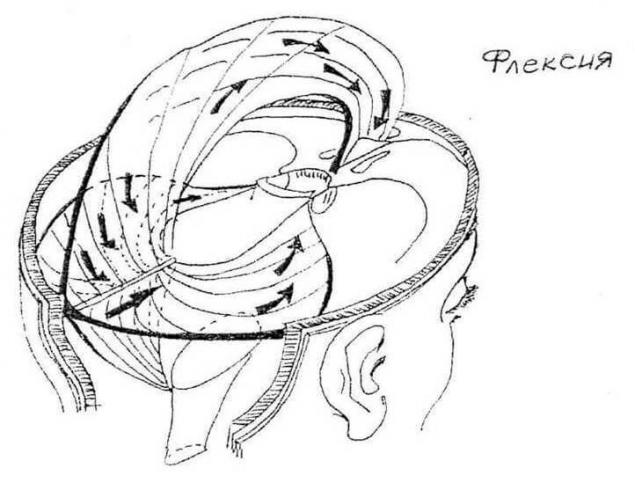
Fig. 3. The cranial membrane of reciprocal tension. Flexion of the reciprocal tension membrane (Magoun H. I. Osteopathic dans le champs cranien. Ed. Sully, 2004).
As you know, the practical training of osteopathy begins with palpation. And I had experience under the guidance of eminent osteopaths feel the movement of the sickle of the brain according to both the first and second models.
In my opinion, the contradictions in the two described models no no. Depending on how we work with the same structure, we will feel those or other movements.
The second model describes the mobility of the sickle of the brain is more liquid. In it we are included in palpation agreement with motelhotel the membrane.
The first model is more biomechanical. We alpinum mobility (mobility) of bones and membranes in a rude craniosacral rhythm.
A little about mailnote and mobility (mobility). All parts of the body to Express primary respiration in the form of mobility and mailnote.
Mobility is the movement of one structure relative to another (e.g., in the joint or seam, or between different bodies). Each structure in the body expresses natural specific pattern craniosacral mobility. This movement occurs solely as a function of the cranial rhythmic impulse.
Mailnote is the internal respiration of the tissues, the movement that arises from within an individual structure. Mailnote is normally expressed in tissues such as the rise up and the extension in hand, then comes back and contraction. Basically it is a factor of the average tide. It is believed that a natural craniosacral mobility occurring between structures, primarily generated by their internal motelhotel (Michael Kern. The wisdom of the body).
At work, when we go deeper palpation of the craniosacral rhythm in the liquid approach, the quality of the movement of the membranes may also go from 1 to 2 describes the model.published by: Oleg Babkin P. S. And remember, only by changing their consumption — together we change the world! ©
Source: osteopatbabkin.blogspot.ru/2013/05/2.html?m=1
Osteopathy, as you know, an exact science. And as in every exact science in osteopathy simultaneously and equally there are two opposing models of the biomechanics of the sickle of the brain. Will try to disassemble both.

The model of mobility of hammer No. 1
This is a rather mechanistic and very logical model, and it consists in the following.
The sickle of the brain, the tent of the cerebellum and other elements of the Dura mater (dura mater pachymeninx) is a system of membranes of reciprocal tension, or Tensegrity (tensegrity). Sometimes in early translations of foreign osteopathic texts, these elements of Dura mater called the reciprocal of the membrane.
A little of the theory of Tensegrity (tensegrity). A system of mutual tension Tensegrity uses free connection of rigid elements. When exposed to such a system (in our case is gravity, PDM) design changes form. Thus there is redistribution of stresses uniformly over all elements of the system. It provides structural strength, and such a system is obtained simultaneously adaptive and resilient.
By changing the position of the skull bones in the phase of the inflections and extensions of the craniosacral rhythm of the reciprocal tension membrane take the position, so that the voltage is evenly redistributed throughout the system TMO. The tension within the membrane is not changed. I.e. the sickle of the brain and the tent of the cerebellum work as inextensible and elastic membrane.
His own mobility at the sickle of the brain in this model, no no. Shifting to the craniosacral rhythm, cranial bones result in movement of the sickle of the brain and the tent of the cerebellum. The direction and form of the displacement of the membranes are defined by axes and vectors craniosacral mobility of the bones to which these membranes are attached.
Further, it is logical to conclude that examining the biomechanics of the bones associated with the hammer and the tent of the cerebellum, we can understand the biomechanics of the hammer and the tent of the cerebellum.

Fig.1. The mobility of the bones of the skull concerned in the movement of the sickle of the brain on the phase of the inflections of the craniosacral rhythm.
1. The sickle of the brain, in its anterior section is attached to the cock the crest of the ethmoid bone.
The movement of the ethmoid bone in the PDM cycle in the sagittal plane:
- The transverse axis (white circle 1) motion passes through the center of the ethmoid bone. The phase of the inflections cockscomb rises cranial. The dorsal part of the bone descends caudally.
The movement of the frontal bone on the phase of the inflections of the craniosacral rhythm in the sagittal plane:
- The transverse axis (white circle 2) traffic passes through the tuberosity of the frontal bone. In the phase of inflection scales of the frontal bone should be dorsal. Bregma and the dorsal scales also lowers slightly caudally. In addition, all metaphase seam a little deeper.
The movement of the parietal bones in the PDM cycle in the sagittal plane:
- The transverse axis (white circle 3) craniosacral mobility passes through the tuberosity of the parietal bone. The phase of the inflections bregma followed by the dorsal, lambda dorsocaudal. In addition, the entire sagittal suture slightly deepened.
The movement of the occipital bone in the PDM cycle in the sagittal plane:
- The transverse axis (white circle 4) movement of the occipital bone passes over the jugular processes at the level of the SBS. The phase of the cranial inflection scales of the occipital bone deviates dorsal and caudal.

Fig.2. Blue arrows show the movement of a large sickle in the phase of the inflections of VSD.
Model 2, when the hammer twists "on itself"
As we know, Sutherland has put forward 5 phenomena of the primary respiratory mechanism. The classical concept of PDM is based on these five principles:
1. Mailnote the brain and spinal cord. 2. Fluctuations of the cerebrospinal fluid.
3. The mobility of the membranes of reciprocal tension.
4. The mobility of the skull bones in joints.
5. Involuntary mobility of the sacrum between the iliac bones.
- A large sickle of the brain is moved anteriorly in the direction of its attachment to the ethmoid bone and is shortened from front to back;
- The tent moves anteriorly, is flattened and expanded;
- System of membranes as a whole moves up and shortened from the top down.
The centre of this movement, or fulcrum is the fulcrum of Sutherland, located in front of the straight sinus. This is a moving, dynamic pivot point that moves its position during the cycles of primary respiration. During the phase of exhalation the opposite happens movement.

Fig. 3. The cranial membrane of reciprocal tension. Flexion of the reciprocal tension membrane (Magoun H. I. Osteopathic dans le champs cranien. Ed. Sully, 2004).
As you know, the practical training of osteopathy begins with palpation. And I had experience under the guidance of eminent osteopaths feel the movement of the sickle of the brain according to both the first and second models.
In my opinion, the contradictions in the two described models no no. Depending on how we work with the same structure, we will feel those or other movements.
The second model describes the mobility of the sickle of the brain is more liquid. In it we are included in palpation agreement with motelhotel the membrane.
The first model is more biomechanical. We alpinum mobility (mobility) of bones and membranes in a rude craniosacral rhythm.
A little about mailnote and mobility (mobility). All parts of the body to Express primary respiration in the form of mobility and mailnote.
Mobility is the movement of one structure relative to another (e.g., in the joint or seam, or between different bodies). Each structure in the body expresses natural specific pattern craniosacral mobility. This movement occurs solely as a function of the cranial rhythmic impulse.
Mailnote is the internal respiration of the tissues, the movement that arises from within an individual structure. Mailnote is normally expressed in tissues such as the rise up and the extension in hand, then comes back and contraction. Basically it is a factor of the average tide. It is believed that a natural craniosacral mobility occurring between structures, primarily generated by their internal motelhotel (Michael Kern. The wisdom of the body).
At work, when we go deeper palpation of the craniosacral rhythm in the liquid approach, the quality of the movement of the membranes may also go from 1 to 2 describes the model.published by: Oleg Babkin P. S. And remember, only by changing their consumption — together we change the world! ©
Source: osteopatbabkin.blogspot.ru/2013/05/2.html?m=1